Supraspinatus muscle
| Supraspinatus muscle | |
|---|---|
 Position of the supraspinatus muscle (red) seen from the back. | |
 Posterior view of muscles connecting the upper extremity to the vertebral column. Supraspinatus muscle is labeled in red at right, while it is covered by other muscles at left. | |
| Details | |
| Origin | supraspinous fossa of scapula |
| Insertion | superior facet of greater tubercle of humerus |
| Artery | suprascapular artery |
| Nerve | suprascapular nerve |
| Actions | abduction of arm and stabilizes humerus see part on controversy of action. |
| Identifiers | |
| Latin | musculus supraspinatus |
| TA | A04.6.02.006 |
| FMA | 9629 |
The supraspinatus (plural supraspinati, from Latin supraspinatus) is a relatively small muscle of the upper back that runs from the supraspinatous fossa superior of the scapula (shoulder blade) to the greater tubercle of the humerus. It is one of the four rotator cuff muscles and also abducts the arm at the shoulder. The spine of the scapula separates the supraspinatus muscle from the infraspinatus muscle, which originates below the spine.
Structure
The supraspinatus muscle arises from the supraspinous fossa, a shallow depression in the body of the scapula above its spine. The supraspinatus muscle tendon passes laterally beneath the cover of the acromion. Research in 1996 showed that the postero-lateral origin was more lateral than classically described.[1][2]
The supraspinatus tendon is inserted into the superior facet of the greater tubercle of the humerus.[3] The distal attachments of the three rotator cuff muscles that insert into the greater tubercle of the humerus can be abbreviated as SIT when viewed from superior to inferior (for supraspinatus, infraspinatus, and teres minor), or SITS when the subscapularis muscle, which attaches to the lesser tubercle of the humerus, is included.[4]
Innervation
The suprascapular nerve (C5)innervates the supraspinatus muscle as well as the infraspinatus muscle. It comes from the upper trunk of the brachial plexus. This nerve can be damaged along its course in fractures of the overlying clavicle, which can reduce the person's ability to initiate the abduction.
Repair
One study has indicated that arthroscopic surgery for full-thickness supraspinatus tears is effective for improving shoulder functionality.[5]
A comparative study performed at the University of Alberta Evidence-based Practice Center in 2010 highlighted multiple key findings regarding the repair of supraspinatus tears. Subjects who received surgical rotator cuff repair early redeveloped superior shoulder function in comparison to the delayed surgical group. In terms of operative techniques, differences in neither cuff integrity nor shoulder function were reported in studies comparing single-row versus double-row suture anchor fixation and mattress locking versus absorbable sutures. Postoperatively, a slight advantage was evident in patients who performed continuous passive motion alongside physical therapy, as opposed to those who solely performed physical therapy. There is insufficient evidence to adequately compare the effects of operative against nonoperative interventions. Complications were reported very seldomly, or were not determined to be clinically significant.[Seida]
A 2016 study evaluating the effectiveness of arthroscopic treatment of rotator cuff calcification firmly supported surgical intervention. Calcification of the supraspinatus tendon is a major contributor to shoulder pain in the general population, and is often worsened following a supraspinatus tear. The results of the study included the return to sports and original functionality of 95.8% of the patients after a mean of 5.3 post-operative months. A significant decrease in pain was observed over time following removal of the calcification. The study showed the overall effectiveness of arthroscopic procedures on shoulder repair, and the lack of risk experienced.[Ranalleta]
Function
Contraction of the supraspinatus muscle leads to abduction of the arm at the shoulder joint. It is the main agonist muscle for this movement during the first 15 degrees of its arc. Beyond 15 degrees the deltoid muscle becomes increasingly more effective at abducting the arm and becomes the main propagator of this action.[6]
The supraspinatus muscle is one of the musculotendinous support structures called the rotator cuff that surround and enclose the shoulder. It helps to resist the inferior gravitational forces placed across the shoulder joint due to the downward pull from the weight of the upper limb.
The supraspinatus also helps to stabilize the shoulder joint by keeping the head of the humerus firmly pressed medially against the glenoid fossa of the scapula.
Without a functioning supraspinatus, the physician must start abducting the patient's arm and eventually the patient will be able to finish abduction if the deltoid is functional, which is common because the supraspinatus is innervated by the suprascapular nerve from the superior/upper trunk of the brachial plexus. The deltoid is innervated more distally by the axillary nerve, which arises from the posterior cord of the brachial plexus.
Controversy about action
In a 1963 experimental human study on the function of the supraspinatus muscle by Van Linge and Mulder at the State University in Leiden, data were provided arguing that the supraspinatus does not cause the first 30 degrees of abduction, as widely accepted before this report, but is, rather, a synergistic muscle that assists the deltoid (but does not abduct alone).[7] In the study, the supraspinati of subjects were anaesthetised; the deltoid muscle remained able to complete a full range of abduction. (However, the deltoid was unable to sustain an isometric contraction for more than one minute.) This study suggested that the "true" action of the supraspinatus is to hold the capsule in position to allow greater functional strength and stamina of the deltoid muscle.
In support of this study, one should also consider the basic mechanics of the forces involved in abduction of the shoulder. The supraspinatus is a smaller and weaker muscle compared to deltoid on three counts: deltoid has three large components (anterior, middle, and posterior fiber groups); the middle fibers have a multipennate arrangement believed to pack more muscle power into a relatively compact space;[8] and it attaches to the deltoid tuberosity halfway down the humerus, adding to the mechanical advantage to abduct the arm. Thus the bulk, arrangement and insertion of the deltoid fibres are designed for the power needed to overcome the load of the weight of the arm plus any load in the hand. By contrast, supraspinatus is a much smaller muscle with convergent fibers leading to a tendon that attaches on the highest facet on the greater tubersosity of the humerus, thereby affording it minimal traction on the arm. The arm is a very long lever with the added weight of muscles and other soft tissues. In 1994, Sharkey and coworkers reported that the whole of the rotator cuff group contributes to abduction of the arm, reducing the work of deltoid by 41%.[9] They strongly suggested that the rotator cuff acts synergistically in concert with deltoid to stabilize the head of the humerus, while the deltoid provides the turning moment at the gleno-humeral joint to abduct the arm. They note that if the deltoid is palpated when abduction is initiated, active contraction of the muscle can be detected—suggesting co-contraction of deltoid with the rotator cuff, rather than after initiation by any of the rotator cuff muscles.
Additional images
 Position of the supraspinatus muscle (shown in red). Animation.
Position of the supraspinatus muscle (shown in red). Animation.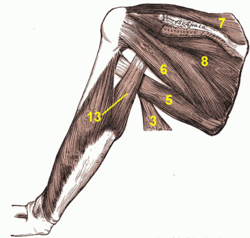 Muscles around the left shoulder, seen from behind.
Muscles around the left shoulder, seen from behind.
3. Latissimus dorsi muscle
5. Teres major muscle
6. Teres minor muscle
7. Supraspinatus muscle
8. Infraspinatus muscle
13. long head of Triceps brachii muscle..gif) Action of right supraspinatus muscle, anterior view. Three bones shown are acromion (top) and coracoid process (center) of scapula, and humerus (left).
Action of right supraspinatus muscle, anterior view. Three bones shown are acromion (top) and coracoid process (center) of scapula, and humerus (left).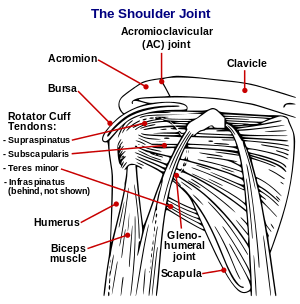 Diagram of the human shoulder joint
Diagram of the human shoulder joint Left scapula. Dorsal surface.
Left scapula. Dorsal surface.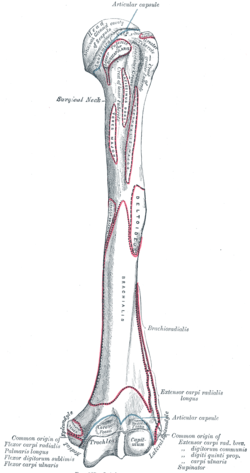 Left humerus. Anterior view.
Left humerus. Anterior view.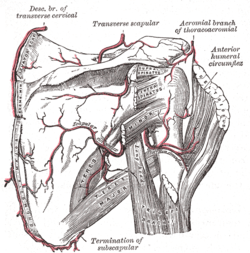 The scapular and circumflex arteries.
The scapular and circumflex arteries. The right brachial plexus with its short branches, viewed from in front.
The right brachial plexus with its short branches, viewed from in front. Suprascapular and axillary nerves of right side, seen from behind.
Suprascapular and axillary nerves of right side, seen from behind. The suprascapular, axillary, and radial nerves.
The suprascapular, axillary, and radial nerves.
References
- ↑ Thomazeau, H.; Duval, J. M.; Darnault, P.; Dréano, T. (1996). "Anatomical relationships and scapular attachments of the supraspinatus muscle". Surgical and Radiologic Anatomy. 18 (3): 221–5. doi:10.1007/BF02346130. PMID 8873337.
- ↑ D.F. Gazielly, P. Gleyze & T. Thomas, 1996, "The Cuff," Elsevier, ISBN 2906077844, see , accessed 21 November 2014.
- ↑ "Injured Shoulder". Retrieved 16 December 2015.
- ↑ MedicalMnemonics.com: 35
- ↑ Bennett, William F. "Arthroscopic Supraspinatus Repair". Bennett Orthopedics & Sportsmedicine. Retrieved 19 December 2014.
- ↑ Gray´s Anatomy for students 3rd edition
- ↑ van Linge, B.; Mulder, J. D. (1963). "Function of the Supraspinatus Muscle and Its Relation to the Supraspinatus Syndrome. An Experimental Study in Man". The Journal of bone and joint surgery. British volume. 45 (4): 750–4. PMID 14074328.
- ↑ Gray's Anatomy 37th Edition 1987
- ↑ Sharkey, Neil A.; Marder, Richard A.; Hanson, Peter B. (1994). "The entire rotator cuff contributes to elevation of the arm". Journal of Orthopaedic Research. 12 (5): 699–708. doi:10.1002/jor.1100120513. PMID 7931787.
- ↑ Seida, J. "Comparitive Effectiveness of Nonoperative and Operative Treatment for Rotator Cuff Tears".
Seida J, Schouten J, Mousavi S, Tjosvold L, Vandermeer B, Milne A, Bond K, Hartling L, LeBlanc C, Sheps D. Comparative Effectiveness of Nonoperative and Operative Treatment for Rotator Cuff Tears. Comparative Effectiveness Review No. 22. (Prepared by the University of Alberta Evidence-based Practice Center under Contract No. 290-02-0023.) AHRQ Publication No. 10-EHC050. Rockville, MD: Agency for Healthcare Research and Quality. July 2010. Available at: www.effectivehealthcare.ahrq.gov/reports/final.cfm.
Ranalletta M, Rossi LA, Sirio A, Bruchmann G, Maignon GD, Bongiovanni SL. Return to Sports After Arthroscopic Treatment of Rotator Cuff Calcifications in Athletes. Orthopaedic Journal of Sports Medicine. 2016;4(10):2325967116669310. doi:10.1177/2325967116669310.
External links
| Wikimedia Commons has media related to Supraspinatus muscles. |