Myocardial bridge
A myocardial bridge occurs when one of the coronary arteries tunnels through the myocardium rather than resting on top of it. Typically, the arteries rest on top of the heart muscle and feed blood down into smaller vessels that populate throughout the myocardium. But if the muscle grows around one of the larger arteries, then a myocardial bridge is formed. As the heart squeezes to pump blood, the muscle exerts pressure across the bridge and constricts the artery. This defect is present from birth. It can lead to uncomfortable, powerful heartbeats and angina. The incidence of the condition in the general population is estimated at 5% based on autopsy findings,[1] but significance when found in association with other cardiac conditions is unknown.[2]
The condition is diagnosed on a scaled based on what percentage of obstruction occurs. If there is less than 50% blockage, then the condition is probably benign. A result of at least 70% usually causes some pain. Small amounts of myocardial bridging often are undetectable, as the blood usually flows through the coronary while the heart is relaxing in diastole.
This condition can cause complications such as vasospasm, angina pectoris, arrhythmia, ventricular tachycardia. Additionally many patients express discomfort in specific positions, (i.e. lying on the left side for a prolonged period of time).
Case study
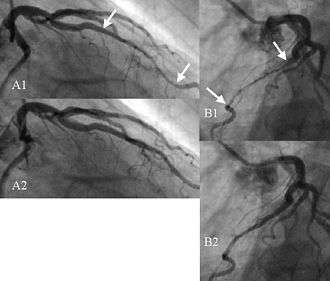
Figure 1 shows a series of angiographic images with a bridge on the left anterior descending coronary artery (LAD) in a male patient of 65 years.
- A1) Right anterior oblique view taken at end systole. The compressed vessel segment is indicated by the two arrows.
- B1) Left anterior oblique view taken nearly at the same instant.
- A2) Same view as in A1, but taken 133 ms later. The tunneled segment is no longer compressed.
- B2) Same view as in B1 but 133 ms later.
Treatment
Surgery for symptomatic myocardial bridge of the LAD may include myotomy, coronary artery bypass surgery, or both.[3] [4] Procedure selection is based on the size of the underlying artery during diastole, the presence of concomitant proximal coronary artery disease, and the presence of anatomic factors that would increase the risk of myotomy. Surgical strategy for the management should be customized, and the treatment of choice is myotomy but bypass surgery can be added when there is proximal coronary obstruction or anatomic anomalies that increase the risk of recurrence of the obstruction.[5]
See also
References
- ↑ Pelliccia, Antonio (2009), Sports Cardiology Casebook, Springer, p. 141, ISBN 978-1-84882-041-8
- ↑ Ragosta, Michael (2009), Cardiac Catheterization: An Atlas and DVD, Elsevier Health Sciences, p. 146, ISBN 978-1-4160-3999-0
- ↑ Bruschke AV, Veltman CE, de Graaf MA, Vliegen HW. Myocardial bridging: what have we learned in the past and will new diagnostic modalities provide new insights? Neth Heart J. 2013;21:6-13
- ↑ Sun X, Chen H, Xia L, Zhao D, Ding W, Wang C. Coronary artery bypass grafting for myocardial bridges of the left anterior descending artery. J Card Surg. 2012;27: 405-7.
- ↑ Ekeke C, Noble S, Mazzaferri E, Crestanello J (2015). "Myocardial bridging over the left anterior descending: Myotomy, bypass, or both?". The Journal of Thoracic and Cardiovascular Surgery. 149: e57–e58. doi:10.1016/j.jtcvs.2014.12.054.
External links
- Harlan Krumholz, M.D. discusses myocardial bridging
- Medical definition of myocardial bridge
- Myocardial bridge summary by the Texas Heart Institute