Medullary sponge kidney
| Medullary sponge kidney | |
|---|---|
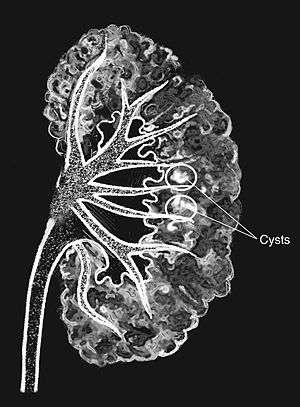 | |
| Medullary sponge as seen on an intravenous pyelogram | |
| Classification and external resources | |
| Specialty | medical genetics, nephrology |
| ICD-10 | Q61.5 |
| ICD-9-CM | 753.17 |
| DiseasesDB | 7915 |
| eMedicine | article/379323 |
| MeSH | D007691 |
Medullary Sponge Kidney (also known as Cacchi–Ricci disease) is a congenital disorder of the kidneys characterized by cystic dilatation of the collecting tubules in one or both kidneys. Individuals with medullary sponge kidney are at increased risk for kidney stones and urinary tract infection. Patients with MSK typically pass twice as many stones per year as do other stone formers without MSK. While described as a "benign" disorder with a low morbidity rate, as many as 10% of patients with MSK have an increased risk of morbidity associated with frequent stones and UTIs. While some patients report increased chronic kidney pain, the source of the pain, when a UTI or blockage is not present, is unclear at this time. Renal colic (flank and back pain) is present in 55% of patients. Women with MSK experience more stones, UTIs and complications than men. MSK was previously believed not to be hereditary but there is more evidence coming forth that may indicate otherwise.[1][2]
Etiology
In recent studies, insight has been obtained on the genetic basis of this disease, supporting the hypothesis that MSK is due to a disruption at the 'ureteric bud-metanephric mesenchyme' interface. This explains why so many tubular defects coexist in this disease, and particularly a distal tubular acidification defect of which the highly prevalent metabolic bone disease is one very important consequence. In addition to the typical clinical phenotype of recurrent stone disease, other clinical profiles have now been recognized, that is, an indolent, almost asymptomatic MSK, and a rare form characterized by intractable, excruciating pain.[3] It was previously believed that most cases of Medullary Sponge Kidney were sporadic however, recent studies show familial clustering of MSK is common, and has an autosomal dominant inheritance, a reduced penetrance, and variable expressivity.[4][5] Other theories suggest that dilatation of a collecting duct may occur, caused by occlusion by uric acid during fetal life or resulting from tubular obstruction due to calcium oxalate calculi secondary to infantile hypercalciuria.[6]
A rare, autosomal recessive form is associated with Caroli disease.[6]
Epidemiology
In the general population, the frequency of medullary sponge kidney disease is reported to be 0.02–0.005%; that is, 1 in 5000 to 1 in 20,000. The frequency of medullary sponge kidney has been reported by various authors to be 12 – 21% in patients with kidney stones (nephrolithiasis).[7] The disease is bilateral in 70% of cases.
Presentation
Most cases are asymptomatic or are discovered during investigation of hematuria. Symptomatic patients typically present as middle aged adults with renal colic, nephrolithiasis, nephrocalcinosis and/or recurrent urinary tract infections; however, MSK also may affect children very rarely. In addition to the typical clinical phenotype of recurrent stone disease, other clinical profiles have now been recognized, that is, an indolent, almost asymptomatic MSK, and a rare form characterized by intractable pain.[8]
Diagnosis
Classically, MSK is seen as hyperdense papillae with clusters of small stones on renal ultrasonography or abdominal x-ray. The irregular (ectatic) collecting ducts often seen in MSK, which are sometimes described as having a "paintbrush-like" appearance, are best seen on intravenous urography. However, IV urography has been largely replaced by contrast-enhanced, high-resolution helical CT with digital reconstruction.[9]
Treatment
Often, aggressive treatment is unnecessary for people with disease that does not cause any symptoms (asymptomatic).[9] In such cases, treatment may consist of maintaining adequate fluid intake, with the goal of decreasing the risk of developing kidney stones (nephrolithiasis).[9] Cases of recurrent kidney stone formation may warrant evaluation for possible underlying metabolic abnormalities.[9]
In patients with low levels of citrate in the urine (hypocitraturia) and incomplete distal renal tubular acidosis, treatment with potassium citrate helps prevent the formation of new kidney stones.[9] Urinary tract infections, when they occur, should also be treated.[9]
Patients with the more rare form of MSK marked by chronic pain typically require pain management. Non-obstructing stones in MSK can be associated with significant and chronic pain even if they're not passing. The pain in this situation can be constant. It is not certain what causes this pain but researchers have proposed that the small numerous stones seen in MSK may cause obstruction of the small tubules and collecting ducts in the kidney which could lead to the pain. This pain can often be debilitating and treatment is challenging. Narcotic medication even with large quantities is sometimes not adequate. Some success with pain control has been reported using laser lithotripsy (called “ureteroscopic laser papillotomy”).[10]
Complications
Complications associated with medullary sponge kidney include the following:
- Renal stones[6]
- Urinary tract infection (UTI)[6]
- Hematuria[6]
- Distal renal tubular acidosis (Type 1 RTA)[6]
- Renal insufficiency (rarely)[6]
- Marked chronic pain[6]
- Chronic kidney failure[6]
Support & Awareness
Many patients with MSK find support in online support groups.
MSK awareness colors are purple, teal and green.

References
- ↑ "Medullary Sponge Kidney". Retrieved 22 August 2012.
- ↑ "Evidence for inheritance of medullary sponge kidney". Retrieved 15 February 2013.
- ↑ Gambaro, Giovanni; Danza, Francesco M.; Fabris, Antonia (July 2013). "Medullary sponge kidney". Current Opinion in Nephrology and Hypertension. 22 (4): 421–426. doi:10.1097/MNH.0b013e3283622b86.
- ↑ Fabris, Antonia; Lupo, Antonio; Ferraro, Pietro M; Anglani, Franca; Pei, York; Danza, Francesco M; Gambaro, Giovanni. "Familial clustering of medullary sponge kidney is autosomal dominant with reduced penetrance and variable expressivity". Kidney International. 83 (2): 272–277. doi:10.1038/ki.2012.378.
- ↑ Goldfarb, David S (February 2013). "Evidence for inheritance of medullary sponge kidney". Kidney International. 83 (2): 193–196. doi:10.1038/ki.2012.417.
- 1 2 3 4 5 6 7 8 9 Ghosh, Amit K. "Medullary Sponge Kidney". Medscape Reference. Retrieved 1 January 2013.
- ↑ Ginalski, JM; Portmann L; Jaeger P (1990). "Does medullary sponge kidney cause nephrolithiasis?" (PDF). American Journal of Roentgenology. 155 (2): 299–302. doi:10.2214/ajr.155.2.2115256. PMID 2115256.
- ↑ "Medullary Sponge Kidney".
- 1 2 3 4 5 6 Salant DJ]; Gordon CE (2012). "Chapter 284. Polycystic Kidney Disease and Other Inherited Tubular Disorders". Harrison's Principles of Internal Medicine. (18th ed.). New York: McGraw-Hill. ISBN 978-0071748896.
- ↑ "What is Medullary Sponge Kidney?". Retrieved 21 May 2014.