Congenital cytomegalovirus infection
| Congenital cytomegalovirus infection | |
|---|---|
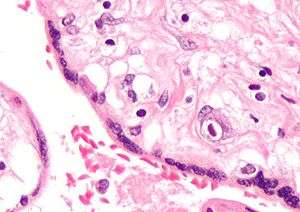 | |
| Micrograph of a cytomegalovirus (CMV) infection of the placenta (CMV placentitis). The characteristic large nucleus of a CMV infected cell is seen off-centre at the bottom-right of the image. H&E stain | |
| Classification and external resources | |
| Specialty | pediatrics |
| ICD-10 | P35.1 |
| ICD-9-CM | 771.1 |
| MedlinePlus | 001343 |
| eMedicine | article/963090 |
Congenital cytomegalovirus infection refers to a condition where cytomegalovirus is transmitted in the prenatal period.
Human cytomegalovirus is one of the vertically transmitted infections that lead to congenital abnormalities. (Others are: toxoplasmosis, rubella, and herpes simplex. )
Epidemiology
Congenital HCMV infection occurs when the mother suffers a primary infection (or reactivation) during pregnancy. Due to the lower seroprevalence of HCMV in industrialized countries and higher socioeconomic groups, congenital infections are actually less common in poorer communities, where more women of child-bearing age are already seropositive. In industrialized countries up to 8% of HCMV seronegative mothers contract primary HCMV infection during pregnancy, of which roughly 50% will transmit to the fetus.[1] Between 22–38% of infected fetuses are then born with symptoms,[2] which may include pneumonia, gastrointestinal, retinal and neurological disease.[3][4] HCMV infection occurs in roughly 1% of all neonates with those who are not congenitally infected contracting the infection possibly through breast milk.[5][6][7] Other sources of neonatal infection are bodily fluids which are known to contain high titres in shedding individuals: saliva (<107copies/ml) and urine (<105copies/ml )[8][9] seem common routes of transmission.
The incidence of primary CMV infection in pregnant women in the United States varies from 1% to 3%. Healthy pregnant women are not at special risk for disease from CMV infection. When infected with CMV, most women have no symptoms and very few have a disease resembling infectious mononucleosis. It is their developing fetuses that may be at risk for congenital CMV disease. CMV remains the most important cause of congenital viral infection in the United States. HCMV is the most common cause of congenital infection in humans and intrauterine primary infections are more common than other well-known infections and syndromes, including Down Syndrome, Fetal Alcohol Syndrome, Spina Bifida, and Pediatric HIV/AIDS.
Presentation
For infants who are infected by their mothers before birth, two potential adverse scenarios exist:
- Generalized infection may occur in the infant, and can cause complications such as low birth weight, microcephaly, seizures, petechial rash similar to the "blueberry muffin" rash of congenital rubella syndrome, and moderate hepatosplenomegaly (with jaundice). Though severe cases can be fatal, with supportive treatment most infants with CMV disease will survive. However, from 80% to 90% will have complications within the first few years of life that may include hearing loss, vision impairment, and varying degrees of mental retardation.
- Another 5% to 10% of infants who are infected but without symptoms at birth will subsequently have varying degrees of hearing and mental or coordination problems. The onset of hearing loss can occur at any point during childhood, although commonly within the first decade. It is progressive and can affect both ears.
These risks appear to be almost exclusively associated with women who previously have not been infected with CMV and who are having their first infection with the virus during pregnancy. There appears to be little risk of CMV-related complications for women who have been infected at least 6 months prior to conception. For this group, which makes up 50% to 80% of the women of child-bearing age, the rate of newborn CMV infection is 1%, and these infants appear to have no significant illness or abnormalities.[10]
The virus can also be transmitted to the infant at delivery from contact with genital secretions or later in infancy through breast milk. However, these infections usually result in little or no clinical illness in the infant.
To summarise, during a pregnancy when a woman who has never had CMV infection becomes infected with CMV, there is a risk that after birth the infant may have CMV-related complications, the most common of which are associated with hearing loss, visual impairment, or diminished mental and motor capabilities. On the other hand, healthy infants and children who acquire CMV after birth have few, if any, symptoms or complications. However, preterm born infants infected with CMV after birth (especially via breastmilk[11]). This can lead to cognitive and motor impairments later in life.[12][13]
Prevention
Recommendations for pregnant women with regard to CMV infection:
- Throughout the pregnancy, practice good personal hygiene, especially handwashing with soap and water, after contact with diapers or oral secretions (particularly with a child who is in day care). Sharing of food, eating and drinking utensils, and contact with toddlers' saliva should be avoided.
- Women who develop a mononucleosis-like illness during pregnancy should be evaluated for CMV infection and counseled about the possible risks to the unborn child.
- Laboratory testing for antibody to CMV can be performed to determine if a woman has already had CMV infection.
- Recovery of CMV from the cervix or urine of women at or before the time of delivery does not warrant a cesarean section.
- The demonstrated benefits of breast-feeding outweigh the minimal risk of acquiring CMV from the breast-feeding mother.
- There is no need to either screen for CMV or exclude CMV-excreting children from schools or institutions because the virus is frequently found in many healthy children and adults.
Treatment with hyperimmune globulin in mothers with primary CMV infection has been shown to be effective in preventing congenital disease in several studies.[14][15][16][17] One study did not show significant decrease in the risk of congenital cytomegalovirus infection.[18]
Childcare
Most healthy people working with infants and children face no special risk from CMV infection. However, for women of child-bearing age who previously have not been infected with CMV, there is a potential risk to the developing unborn child (the risk is described above in the Pregnancy section). Contact with children who are in day care, where CMV infection is commonly transmitted among young children (particularly toddlers), may be a source of exposure to CMV. Since CMV is transmitted through contact with infected body fluids, including urine and saliva, child care providers (meaning day care workers, special education teachers, as well as mothers) should be educated about the risks of CMV infection and the precautions they can take.[19] Day care workers appear to be at a greater risk than hospital and other health care providers, and this may be due in part to the increased emphasis on personal hygiene in the health care setting.
Recommendations for individuals providing care for infants and children:
- Employees should be educated concerning CMV, its transmission, and hygienic practices, such as handwashing, which minimize the risk of infection.
- Susceptible nonpregnant women working with infants and children should not routinely be transferred to other work situations.
- Pregnant women working with infants and children should be informed of the risk of acquiring CMV infection and the possible effects on the unborn child.
- Routine laboratory testing for CMV antibody in female workers is not specifically recommended due to its high occurrence, but can be performed to determine their immune status.
CMV Testing and Diagnosis
People infected with CMV develop antibodies to it, initially IgM later IgG indicating current infection and immunity respectively. If the virus is detected in the blood, saliva, urine or other body tissues, it means that the person has an active infection.
When infected with CMV, most women have no symptoms, but some may have symptoms resembling mononucleosis. Women who develop a mononucleosis-like illness during pregnancy should consult their medical provider.
The Centers for Disease Control and Prevention (CDC) does not recommend routine maternal screening for CMV infection during pregnancy because there is no test that can definitively rule out primary CMV infection during pregnancy. Women who are concerned about CMV infection during pregnancy should practice CMV prevention measures.Considering that the CMV virus is present in saliva, urine, tears, blood, mucus, and other bodily fluids, frequent hand washing with soap and water is important after contact with diapers or oral secretions, especially with a child who is in daycare or interacting with other young children on a regular basis.
A diagnosis of congenital CMV infection can be made if the virus is found in an infant's urine, saliva, blood, or other body tissues during the first week after birth. Antibody tests cannot be used to diagnose congenital CMV; a diagnosis can only be made if the virus is detected during the first week of life. Congenital CMV cannot be diagnosed if the infant is tested more than one week after birth.
Visually healthy infants are not routinely tested for CMV infection although only 10–20% will show signs of infection at birth though up to 80% may go onto show signs of prenatal infection in later life. If a pregnant woman finds out that she has become infected with CMV for the first time during her pregnancy, she should have her infant tested for CMV as soon as possible after birth.
References
- ↑ Adler SP (December 2005). "Congenital cytomegalovirus screening". Pediatr. Infect. Dis. J. 24 (12): 1105–6. doi:10.1097/00006454-200512000-00016. PMID 16371874.
- ↑ Griffiths PD, Walter S (June 2005). "Cytomegalovirus". Curr. Opin. Infect. Dis. 18 (3): 241–5. doi:10.1097/01.qco.0000168385.39390.1b. PMID 15864102.
- ↑ Barry Schoub; Zuckerman, Arie J.; Banatvala, Jangu E.; Griffiths, Paul E. (2004). "Chapter 2C Cytomegalovirus". Principles and Practice of Clinical Virology. Chichester: John Wiley & Sons. pp. 85–122. ISBN 0-470-84338-1.
- ↑ Vancíková Z, Dvorák P (2001). "Cytomegalovirus infection in immunocompetent and immunocompromised individuals--a review". Curr. Drug Targets Immune Endocr. Metabol. Disord. 1 (2): 179–87. doi:10.2174/1568008013341334. PMID 12476798.
- ↑ Kerrey BT, Morrow A, Geraghty S, Huey N, Sapsford A, Schleiss MR (2006). "Breast milk as a source for acquisition of cytomegalovirus (HCMV) in a premature infant with sepsis syndrome: detection by real-time PCR". J. Clin. Virol. 35 (3): 313–6. doi:10.1016/j.jcv.2005.09.013. PMID 16300992.
- ↑ Schleiss MR; Dror, Yigal (2006). "Role of breast milk in acquisition of cytomegalovirus infection: recent advances". Curr. Opin. Pediatr. 18 (1): 48–52. doi:10.1097/01.mop.0000192520.48411.fa. PMID 16470162.
- ↑ Schleiss MR (2006). "Acquisition of human cytomegalovirus infection in infants via breast milk: natural immunization or cause for concern?". Rev. Med. Virol. 16 (2): 73–82. doi:10.1002/rmv.484. PMID 16287195.
- ↑ Kearns AM, Turner AJ, Eltringham GJ, Freeman R (2002). "Rapid detection and quantification of CMV DNA in urine using LightCycler-based real-time PCR". J. Clin. Virol. 24 (1–2): 131–4. doi:10.1016/S1386-6532(01)00240-2. PMID 11744437.
- ↑ Yoshikawa T, Ihira M, Taguchi H, Yoshida S, Asano Y (2005). "Analysis of shedding of 3 beta-herpesviruses in saliva from patients with connective tissue diseases". J. Infect. Dis. 192 (9): 1530–6. doi:10.1086/496890. PMID 16206067.
- ↑ Ryan KJ, Ray CG, eds. (2004). Sherris Medical Microbiology (4th ed.). McGraw Hill. pp. 556; 566–9. ISBN 0-8385-8529-9.
- ↑ Maschmann, J.; Hamprecht, K.; Dietz, K.; Jahn, G.; Speer, C. P. (2001). "Cytomegalovirus Infection of Extremely Low—Birth Weight Infants via Breast Milk". Clinical Infectious Diseases. pp. 1998–2003. doi:10.1086/324345.
- ↑ Brecht, Katharina; Goelz, Rangmar; Bevot, Andrea; Krägeloh- Mann, Ingeborg; Wilke, Marko; Lidzba, Karen. "Postnatal Human Cytomegalovirus Infection in Preterm Infants Has Long-Term Neuropsychological Sequelae". Journal of Pediatrics. Retrieved 5 August 2016.
- ↑ Bevot, Andrea; Hamprecht, Klaus; Krägeloh-Mann, Ingeborg; Brosch, Sibylle; Goelz, Rangmar; Vollmer, Brigitte (1 April 2012). "Long-term outcome in preterm children with human cytomegalovirus infection transmitted via breast milk". Acta Paediatrica. pp. e167–e172. doi:10.1111/j.1651-2227.2011.02538.x.
- ↑ Nigro, G.; Adler, S.P.; La Torre, R.; Best, A.M. (2005). "Passive immunization during pregnancy for congenital cytomegalovirus infection.". N. Engl. J. Med. 353: 1350–1362. doi:10.1056/nejmoa043337.
- ↑ Visentin, S.; Manara, R.; Milanese, L.; Da Roit, A.; Salviato, E.; Citton, V.; Magno, F.M.; Morando, C. (2012). "Early primary cytomegalovirus infection in pregnancy: maternal hyperimmunoglobulin therapy improves outcomes among infants at 1 year of age.". Clin Infect Dis. 55: 497–503. doi:10.1093/cid/cis423.
- ↑ Nigro, G.; Adler, S.P.; Parruti, G.; Anceschi, M.M.; Coclite, E.; pezone, I.; Di Renzo, G.C. (2012). "Immunoglobulin therapy of fetal cytomegalovirus infection occurring in the first half of pregnancy--a case-control study of the outcome in children.". J Infect Dis. 205: 215–227. doi:10.1093/infdis/jir718.
- ↑ Buxmann, H.; Stackelberg, O.M.; Schlosser, R.L.; Enders, G.; Gonser, M.; Meyer-Wittkopf, M.; Hamprecht, K.; Enders, M. (2012). "Use of cytomegalovirus hyperimmunoglobulin for prevention of congenital cytomegalovirus disease: a retrospective analysis.". J Perinat Med: 439–446.
- ↑ Revello, M. G.; Lazzarotto, T.; Guerra, B.; Spinillo, A.; Ferrazzi, E.; Kustermann, A.; Guaschino, S.; Vergani, P.; Todros, T.; Frusca, T.; Arossa, A.; Furione, M.; Rognoni, V.; Rizzo, Nicola; Gabrielli, Liliana; Klersy, Catherine; Gerna, G. (2014). "A Randomized Trial of Hyperimmune Globulin to Prevent Congenital Cytomegalovirus". N Engl J Med. 370 (14): 1316–1326. doi:10.1056/NEJMoa1310214. ISSN 0028-4793. PMID 24693891.
- ↑ Pickering, Larry; Baker, Carol; Kimberlin, David; Long, Sarah (2012). 2012 Report of the Committee on Infectious Diseases (PDF) (29 ed.). Elk Grove Village, IL: American Academy of Pediatrics. p. 145. ISBN 978-1-58110-703-6. Retrieved 20 November 2016.
External links
- Cytomegalovirus (CMV)—NHS Choices
- CMV: Congenital CMV Infection—CDC