Astigmatism
| Astigmatism | |
|---|---|
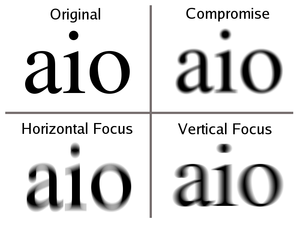
|
Blur from astigmatic lens at different distances | |
| Classification and external resources | |
| Specialty | Ophthalmology |
| ICD-10 | H52.2 |
| ICD-9-CM | 367.2 |
| OMIM | 603047 |
| DiseasesDB | 29648 |
| MedlinePlus | 001015 |
| MeSH | D001251 |
Astigmatism is a type of refractive error in which the eye does not focus light evenly on the retina.[1] This results in distorted or blurred vision at all distances. Other symptoms can include eyestrain, headaches, and trouble driving at night.[1] If it occurs early in life it can result in amblyopia.[2]
The cause of astigmatism is unclear.[3] It is believed to be partly related to genetic factors.[4] The underlying mechanism involves an irregular curvature of the cornea or abnormalities in the lens of the eye.[1][3] Diagnosis is by an eye exam.[1]
Three options exist for the treatment: glasses, contact lenses, and surgery. Glasses are the simplest. Contact lenses can provide a wider field of vision. Refractive surgery permanently changes the shape of the eye.[1]
In Europe and Asia astigmatism affects between 30 and 60% of adults.[4] People of all ages can be affected.[1] Astigmatism was first reported by Thomas Young in the early 1800s.[3]
Signs and symptoms
Although astigmatism may be asymptomatic, higher degrees of an astigmatism may cause symptoms such as blurry vision, squinting, eye strain, fatigue, or headaches.[5] Some research has pointed to the link between astigmatism and higher prevalence of migraine headaches.[6]
Types
.png)
Axis of the principal meridian
- Regular astigmatism – principal meridians are perpendicular.
- With-the-rule astigmatism – the vertical meridian is steepest (a rugby ball or American football lying on its side).[7]
- Against-the-rule astigmatism – the horizontal meridian is steepest (a rugby ball or American football standing on its end).[7]
- Oblique astigmatism – the steepest curve lies in between 120 and 150 degrees and 30 and 60 degrees.[7]
- Irregular astigmatism – principal meridians are not perpendicular.
In with-the-rule astigmatism, a minus cylinder is placed in the horizontal axis to correct the refractive error (or a plus cylinder in the vertical axis). Adding a minus cylinder in the horizontal axis makes the horizontal axis "steeper" (or better: makes the vertical axis "less steep") which makes both axes equally "steep". In against-the-rule astigmatism, a plus cylinder is added in the horizontal axis (or a minus cylinder in the vertical axis).
Axis is always recorded as an angle in degrees, between 0 and 180 degrees in a counter-clockwise direction. Both 0 and 180 degrees lie on a horizontal line at the level of the centre of the pupil, and as seen by an observer, 0 lies on the right of both the eyes.
Focus of the principal meridian
With accommodation relaxed:
- Simple astigmatism
- Compound astigmatism
- Mixed astigmatism – focal lines are on both sides of the retina (straddling the retina)
Throughout the eye
Astigmatism, whether it is regular or irregular, is caused by some combination of external (corneal surface) and internal (posterior corneal surface, human lens, fluids, retina, and eye-brain interface) optical properties. In some people, the external optics may have the greater influence, and in other people, the internal optics may predominate. Importantly, the axes and magnitudes of external and internal astigmatism do not necessarily coincide, but it is the combination of the two that by definition determines the overall optics of the eye. The overall optics of the eye are typically expressed by a person's refraction; the contribution of the external (anterior corneal) astigmatism is measured through the use of techniques such as keratometry and corneal topography. One method analyzes vectors for planning refractive surgery such that the surgery is apportioned optimally between both the refractive and topographic components.[8][9]
Diagnosis
A number of tests are used during eye examinations to determine the presence of astigmatism and to quantify its amount and axis. A Snellen chart or other eye charts may initially reveal reduced visual acuity. A keratometer may be used to measure the curvature of the steepest and flattest meridians in the cornea's front surface.[10] Corneal topography may also be used to obtain a more accurate representation of the cornea's shape.[11] An autorefractor or retinoscopy may provide an objective estimate of the eye's refractive error and the use of Jackson cross cylinders in a phoropter or trial frame may be used to subjectively refine those measurements.[12][13][14] An alternative technique with the phoropter requires the use of a "clock dial" or "sunburst" chart to determine the astigmatic axis and power.[15][16] A keratometer may also be used to estimate astigmatism by finding the difference in power between the two primary meridians of the cornea. Javal's rule can then be used to compute the estimate of astigmatism.
A method of astigmatism analysis by Alpins may be used to determine both how much surgical change of the cornea is needed and after surgery to determine how close treatment was to the goal.[17]
Another rarely used refraction technique involves the use of a stenopaic slit (a thin slit aperture) where the refraction is determined in specific meridians – this technique is particularly useful in cases where the patient has a high degree of astigmatism or in refracting patients with irregular astigmatism.
There are three primary types of astigmatism: myopic astigmatism, hyperopic astigmatism and mixed astigmatism.
Treatment
Astigmatism may be corrected with eyeglasses, contact lenses, or refractive surgery. Various considerations involving eye health, refractive status, and lifestyle determine whether one option may be better than another. In those with keratoconus, certain contact lenses often enable patients to achieve better visual acuity than eyeglasses. Once only available in a rigid, gas-permeable form, toric lenses are now available also as soft lenses.
Laser eye surgery (LASIK and PRK) is successful in treating astigmatism.[18]
Epidemiology
According to an American study nearly three in 10 children (28.4%) between the ages of five and 17 have astigmatism.[19] A recent Brazilian study found that 34% of the students in one city were astigmatic.[20] Regarding the prevalence in adults, a recent study in Bangladesh found that nearly 1 in 3 (32.4%) of those over the age of 30 had astigmatism.[21]
A Polish study published in 2005 revealed "with-the-rule astigmatism" may lead to the onset of myopia.[22]
A number of studies have found the prevalence of astigmatism increases with age.[23]
History
As a student, Thomas Young discovered that he had problems with one eye in 1793.[24] In the following years he did research on his vision problems.[25] He presented his findings in a Bakerian Lecture in 1801.[26]
Independent from Young, George Biddell Airy discovered the phoneme of astigmatism on his own eye.[27] Airy presented his observations on his own eye in February 1825 at the Cambridge Philosophical Society.[28][29] Airy produced lenses to correct his vision problems by 1825,[30] [31] while other sources put this into 1827[32] when Airy obtained cylindrical lenses from an optitian from Ipswich.[33] The name for the condition was not given by Airy, but from William Whewell.[34][35][36]
By the 1860s astigmatism was a well established concept in ophthalmology,[37] and chapters in books described the discovery of astigmatism.[38][39]
References
- 1 2 3 4 5 6 "Facts About Astigmatism". NEI. October 2010. Retrieved 29 September 2016.
- ↑ Harvey, EM (June 2009). "Development and treatment of astigmatism-related amblyopia.". Optometry and vision science : official publication of the American Academy of Optometry. 86 (6): 634–9. PMID 19430327.
- 1 2 3 Read, SA; Collins, MJ; Carney, LG (January 2007). "A review of astigmatism and its possible genesis.". Clinical & experimental optometry. 90 (1): 5–19. PMID 17177660.
- 1 2 Mozayan, E; Lee, JK (July 2014). "Update on astigmatism management.". Current opinion in ophthalmology. 25 (4): 286–90. PMID 24837578.
- ↑ "Astigmatism". MedicineNet. OnHealth.com. Retrieved 8 September 2013.
- ↑ Harle, Deacon E.; Evans, Bruce J. W. (2006). "The Correlation Between Migraine Headache and Refractive Errors". Optometry and Vision Science. 83 (2): 82–7. doi:10.1097/01.opx.0000200680.95968.3e. PMID 16501409.
- 1 2 3 "Astigmatism". Buzzle. Retrieved 21 June 2008.
- ↑ Alpins, NA (1997). "New method of targeting vectors to treat astigmatism". Journal of cataract and refractive surgery. 23 (1): 65–75. doi:10.1016/s0886-3350(97)80153-8. PMID 9100110.
- ↑ Alpins, NA (1997). "Vector analysis of astigmatism changes by flattening, steepening, and torque". Journal of cataract and refractive surgery. 23 (10): 1503–14. doi:10.1016/s0886-3350(97)80021-1. PMID 9456408.
- ↑ "Keratometry". St. Luke's Cataract & Laser Institute. Retrieved 8 September 2013.
- ↑ Corneal Topography and Imaging at eMedicine
- ↑ Graff, T (1962). "Control of the determination of astigmatism with the Jackson cross cylinder". Klinische Monatsblätter für Augenheilkunde und für augenärztliche Fortbildung. 140: 702–8. PMID 13900989.
- ↑ Del Priore, LV; Guyton, DL (1986). "The Jackson cross cylinder. A reappraisal". Ophthalmology. 93 (11): 1461–5. doi:10.1016/s0161-6420(86)33545-0. PMID 3808608.
- ↑ Brookman, KE (1993). "The Jackson crossed cylinder: Historical perspective". Journal of the American Optometric Association. 64 (5): 329–31. PMID 8320415.
- ↑ "Basic Refraction Procedures". Quantum Optical. Retrieved 8 September 2013.
- ↑ "Introduction to Refraction". Nova Southeastern University. Retrieved 8 September 2013.
- ↑ Boyd, Benjamin F. (2011). Modern Ophthalmology The Highlights. Panama: Jaypee Brothers Medical Pub. p. 388. ISBN 9789962678168.
- ↑ Azar, Dimitri T. (2007). Refractive surgery (2nd ed.). Mosby Elsevier. ISBN 9780323035996.
- ↑ Kleinstein, R. N.; Jones, LA; Hullett, S; et al. (2003). "Refractive Error and Ethnicity in Children". Archives of Ophthalmology. 121 (8): 1141–7. doi:10.1001/archopht.121.8.1141. PMID 12912692.
- ↑ Garcia, Carlos Alexandre de Amorim; Oréfice, Fernando; Nobre, Gabrielle Fernandes Dutra; Souza, Dilene de Brito; Rocha, Marta Liliane Ramalho; Vianna, Raul Navarro Garrido (2005). "Prevalence of refractive errors in students in Northeastern Brazil". Arquivos Brasileiros de Oftalmologia. 68 (3): 321–5. doi:10.1590/S0004-27492005000300009. PMID 16059562.
- ↑ Bourne, R; Dineen, BP; Ali, SM; Noorul Huq, DM; Johnson, GJ (2004). "Prevalence of refractive error in Bangladeshi adults*1Results of the National Blindness and Low Vision Survey of Bangladesh". Ophthalmology. 111 (6): 1150–60. doi:10.1016/j.ophtha.2003.09.046. PMID 15177965.
- ↑ Czepita, D; Filipiak, D (2005). "The effect of the type of astigmatism on the incidence of myopia". Klinika oczna. 107 (1–3): 73–4. PMID 16052807.
- ↑ Asano, Kazuko; Nomura, Hideki; Iwano, Makiko; Ando, Fujiko; Niino, Naoakira; Shimokata, Hiroshi; Miyake, Yozo (2005). "Relationship Between Astigmatism and Aging in Middle-aged and Elderly Japanese". Japanese Journal of Ophthalmology. 49 (2): 127–33. doi:10.1007/s10384-004-0152-1. PMID 15838729.
- ↑ Coggin, David (1893). "Notes on the Centennial Anniversary of the Discovery of Astigmatism". Boston Med Surg J. 128: 136–137. doi:10.1056/NEJM189302091280603.
- ↑ Atchison, David A; Charman, W Neil (2011). "Thomas Young's contributions to geometrical optics". Clinical and Experimental Optometry: no. doi:10.1111/j.1444-0938.2010.00560.x.
- ↑ Thomas Young (1801). "Philosophical transactions of the Royal Society of London". Philosophical Transactions of the Royal Society of London. 91: 23–88. doi:10.1098/rstl.1801.0004.
- ↑ Levene, J. R. (1966). "Sir George Biddell Airy, F.R.S. (1801-1892) and the Discovery and Correction of Astigmatism". Notes and Records of the Royal Society of London. 21 (2): 180–199. doi:10.1098/rsnr.1966.0017.
- ↑ Wang, Ming (2007-10-22). Irregular Astigmatism: Diagnosis and Treatment. ISBN 9781556428395.
- ↑ George Biddell Airy (1827). "On a peculiar Defect in the Eye, and a mode of correcting it". Transactions of the Cambridge Philosophical Society.
- ↑ http://rsnr.royalsocietypublishing.org/content/21/2/180. Missing or empty
|title=(help) - ↑ Read, Scott A; Collins, Michael J; Carney, Leo G (2007). "A review of astigmatism and its possible genesis". Clinical and Experimental Optometry. 90 (1): 5. doi:10.1111/j.1444-0938.2007.00112.x. PMID 17177660.
- ↑ Porter, Jason (2006). Adaptive optics for vision science: principles, practices, design, and applications. ISBN 9780471679417.
- ↑ Wood, Alexander; Oldham, Frank. Thomas Young Natural Philosopher 1773-1829.
- ↑ Donders, Franciscus Cornelis (1866). Die Anomalien der Refraction und Accommodation des Auges.
- ↑ Wang, Ming (2007-10-22). Irregular Astigmatism: Diagnosis and Treatment. ISBN 9781556428395.
- ↑ "The Rev. Mr. Goodrich and His Visual Problem" (PDF).
- ↑ Bumstead, J. F. (1863). "A Few Remarks on Astigmatism". Boston Med Surg J. 69: 280–284. doi:10.1056/NEJM186311050691404.
- ↑ Donders, Franciscus C (1862). Astigmatismus und cylindrische Gläser.
- ↑ Artal, Pablo; Tabernero, Juan (2010). "Optics of human eye: 400 years of exploration from Galileo's time". Applied Optics. 49 (16): D123. doi:10.1364/AO.49.00D123. PMID 20517354.
External links
| Look up astigmatism in Wiktionary, the free dictionary. |
- Astigmatism at DMOZ