Lissencephaly
| Lissencephaly | |
|---|---|
 | |
| Lissencephalic brain of human. Lacking surface convolutions (Gyrification). | |
| Classification and external resources | |
| Specialty | medical genetics |
| ICD-10 | Q04.3 |
| ICD-9-CM | 742.2 |
| OMIM | 607432 601545 247200 300121 236670 253800 253280 257320 611603 300215 |
| DiseasesDB | 29492 |
| MeSH | D054082 |
| GeneReviews | |
| Orphanet | 48471 |
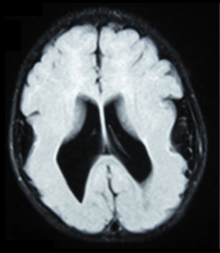
Lissencephaly, which literally means smooth brain, is a rare brain formation disorder caused by defective neuronal migration during the 12th to 24th weeks of gestation resulting in a lack of development of brain folds (gyri) and grooves (sulci).[1] It is a form of cephalic disorder. Terms such as 'agyria' (no gyri) or 'pachygyria' (broad gyri) are used to describe the appearance of the surface of the brain. Children with lissencephaly generally have significant developmental delays, but these vary greatly from child to child depending on the degree of brain malformation and seizure control. Life expectancy can be shortened, generally due to respiratory problems.
Symptoms
Affected children display severe psychomotor retardation, failure to thrive, seizures, and muscle spasticity or hypotonia.[2] Other symptoms of the disorder may include unusual facial appearance, difficulty swallowing, and anomalies of the hands, fingers, or toes.
Diagnosis
The diagnosis of lissencephaly is usually made at birth or soon after by ultrasound,[3] computed tomography (CT), or magnetic resonance imaging (MRI).[4] However, these results should be interpreted cautiously since even experienced radiologists can misdiagnose polymicrogyria, a different developmental malformation of the brain, as lissencephaly.
Before birth, complex ultrasounds performed routinely during pregnancy may indicate the presence of cerebral abnormality, but this method of diagnosis should be complemented by other methods, such as genetic studies and NMR, and the examination is not recommended as part of routine ultrasound examinations, unless family medical history or other reasons for suspecting brain malformation are present. The earliest point during gestation when it is possible to observe abnormal development of the brain surface is approximately in week 20, although ultrasound examinations in week 25–30 are more common.[5] Up to this time, the fetal brain normally has a smooth appearance.[6] If lissencephaly is suspected, chorionic villus sampling can test for some lissencephaly variants, but only those with a known genetic mutation.
Causes
Causes of lissencephaly can include viral infections of the uterus or the fetus during the first trimester,[7] or insufficient blood supply to the fetal brain early in pregnancy. There are also a number of genetic causes of lissencephaly, including mutation of the reelin gene (on chromosome 7),[8] as well as other genes on the X chromosome and on chromosome 17. Genetic counseling is usually offered if there is a risk of lissencephaly, coupled with genetic testing.
Classification
The spectrum of lissencephaly is only now becoming more defined as neuroimaging and genetics have provided more insights into migration disorders. There are around 20 types of lissencephaly which make up the spectrum. Other causes which have not yet been identified are likely as well.
Different systems for classifying lissencephaly exist. One major distinction is "classic" (type I) vs. "cobblestone" (type II),[9] but some systems add additional forms that fit into neither of these categories.
Some types of lissencephaly are described below (OMIM numbers are included where available):
| Category | Types |
| Classic (or Type 1) lissencephaly – 607432 |
|
| Cobblestone (or Type 2) lissencephaly |
|
| Other types |
|
Treatment
Treatment for those with lissencephaly is symptomatic and depends on the severity and locations of the brain malformations. Supportive care may be needed to help with comfort and nursing needs. Seizures may be controlled with medication and hydrocephalus may require shunting. If feeding becomes difficult, a gastrostomy tube may be considered.
Prognosis
The prognosis for children with lissencephaly varies depending on the malformation. Many individuals remain in a 3–5 month developmental level, while others may appear to have near normal intelligence and development. Some children with lissencephaly will be able to roll over, sit, reach for objects, and smile socially. Aspiration and respiratory disease are the most common causes of illness or death.[13] In the past, life expectancy was said to be around two years of age. However, with advances in seizure control, and treatments for respiratory illness, most children live well beyond that age. With other advances in therapy, and the broader availability of services and equipment, some children with lissencephaly are able to walk with varying degrees of assistance and to perform other functions once thought too advanced.
See also
References
- ↑ Dobyns WB (1987). "Developmental aspects of lissencephaly and the lissencephaly syndromes". Birth Defects Orig. Artic. Ser. 23 (1): 225–41. PMID 3472611.
- ↑ Jones, KL (2006). Smith's Recognizable Patterns of Human Malformation (6th ed.). Philadelphia: Elsevier Saunders.
- ↑ Aslan, H; Gungorduk, K; et al. (2009). "Prenatal diagnosis of lissencephaly: a case report.". J Clin Ultrasound. 37 (4): 245–8. doi:10.1002/jcu.20572. PMID 19260111.
- ↑ Cordes, M; Cordes, I; et al. (1988). "Lissencephaly: Diagnosis by computed tomography and magnetic resonance imaging.". Eur J Radiol. 8 (2): 131–3. PMID 3383858.
- ↑ Ghai, Sandeep; Fong, Katherine W; et al. (2006). "Prenatal US and MR Imaging Findings of Lissencephaly: Review of Fetal Cerebral Sulcal Development". RadioGraphics. 26 (2): 389–405. doi:10.1148/rg.262055059. PMID 16549605.
- ↑ Dorovini-Zis K, Dolman CL (April 1977). "Gestational development of brain". Arch. Pathol. Lab. Med. 101 (4): 192–5. PMID 576786.
- ↑ Leena, Dennis Joseph; Pushpalatha; Kuruvilla, Sarah (2008). "Cytomegalovirus infection with lissencephaly". Indian J Pathol Microbiol. 51 (3): 402–4. doi:10.4103/0377-4929.42534. PMID 18723971.
- ↑ Hong SE, Shugart YY, Huang DT, et al. (September 2000). "Autosomal recessive lissencephaly with cerebellar hypoplasia is associated with human RELN mutations". Nat. Genet. 26 (1): 93–6. doi:10.1038/79246. PMID 10973257.
- ↑ Forman MS, Squier W, Dobyns WB, Golden JA (October 2005). "Genotypically defined lissencephalies show distinct pathologies". J. Neuropathol. Exp. Neurol. 64 (10): 847–57. doi:10.1097/01.jnen.0000182978.56612.41. PMID 16215456.
- ↑ Chong, SS; Pack, SD; Roschke, AV; Tanigami, A; Carrozzo, R; Smith, AC; Dobyns, WB; Ledbetter, DH (February 1997). "A revision of the lissencephaly and Miller-Dieker syndrome critical regions in chromosome 17p13.3.". Human Molecular Genetics. 6 (2): 147–55. doi:10.1093/hmg/6.2.147. PMID 9063734.
- ↑ Norman, MG; Roberts, M; Sirois, J; Tremblay, LJ (February 1976). "Lissencephaly.". The Canadian journal of neurological sciences. Le journal canadien des sciences neurologiques. 3 (1): 39–46. PMID 175907.
- ↑ Microlissencephaly
- ↑ Baker, Lisa. "Lissencephaly". The Resource Foundation for Children with Challenges. Retrieved 10 May 2013.
External links
| Wikimedia Commons has media related to Lissencephaly. |
- lissencephaly at NINDS
- Cortical Foundation (support)
- Lissencephaly Launch Pad (support)
- Lissencephaly, generic term (pdf document) – concise and thorough classification of lissencephaly by prof. Alan Verloes.
- GeneReviews/NCBI/NIH/UW entry on DCX-Related Disorders
- OMIM entries on DCX-Related Disorders
- GeneReview/NIH/UW entry on LIS1 Lissencephaly
- MRI Imaging Lissencephaly/Agyria